Who is Choosing Abortion in America?
After 50 years of Roe, the practices of gathering accurate statistics on abortion is still neither uniform, nor comprehensive. This report uses the best statistical reporting available relying upon research from the U.S. Center for Disease Control (CDC), the Kaiser Family Foundation, the Guttmacher Institute (aligned with Planned Parenthood), Pew Research, and reporting agencies from individual state governments. At this time, not all state governments report abortion statistics in a uniform fashion.
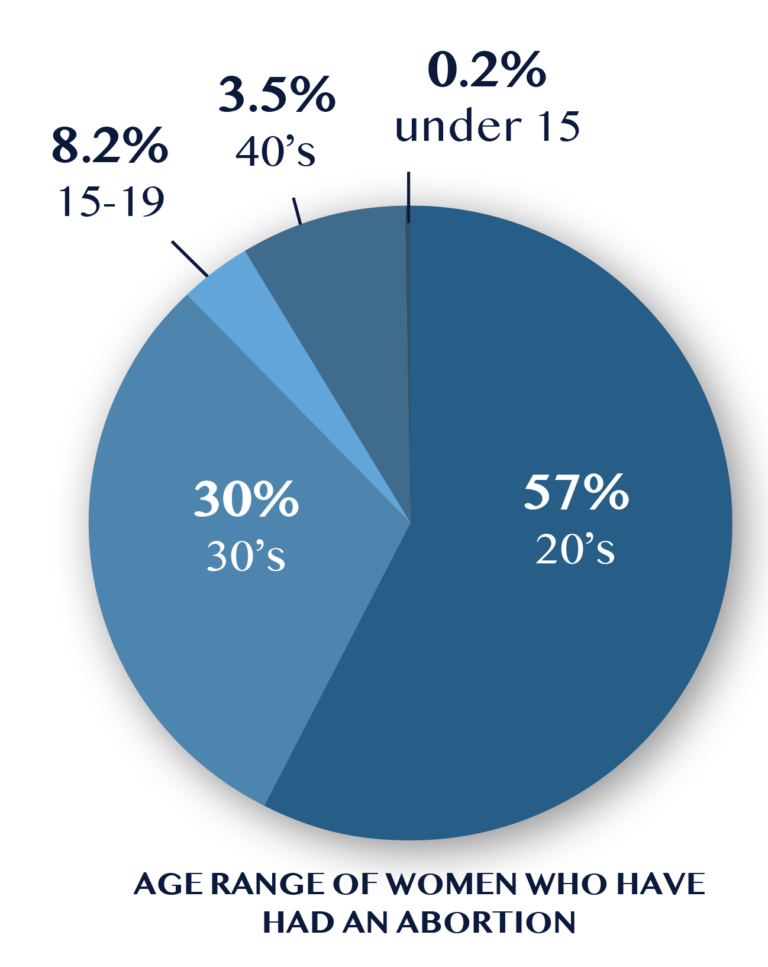
By Age
- 0.2% under the age of 15
- 8.2% ages 15-19
- 57% ages 20-29
- 30% ages 30-39
- 3.5% ages 40-49
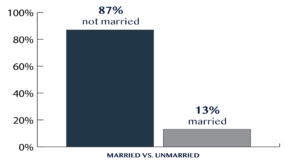
Marital Status
Unmarried women got 87% of all known abortions in 2021, while 13% were married women.
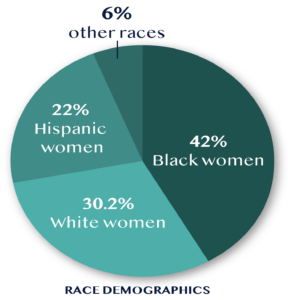
By Race
Accumulated data by the CDC from 31 states that reported racial and ethnic data, New York City and the District of Columbia, shows this distribution:
- 42% Black women
- 30.2% White women
- 22% Hispanic women
- 6% Other races
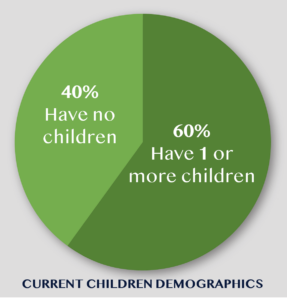
Current Children
- 60% of women who have had an abortion have one or more children
- 40% of women who have had an abortion have no children
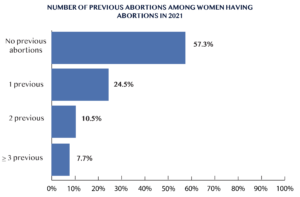
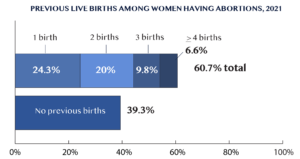
Previous Live Births
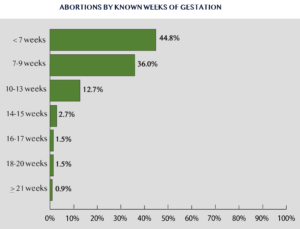
When Are Abortions Performed?
- 40% — First 6 weeks of pregnancy
- 39% — Between 7 and 9 weeks of pregnancy
- 14% — By the end of 13 weeks Approximately
- 7% of abortions occur after the first trimester of pregnancy.
What is the Definition of Abortion in America Today?
For the purposes of law: Abortion is a medical procedure designed to terminate a living pregnancy. This procedure is different than medical treatment for a miscarriage, where the pregnancy has already been lost.
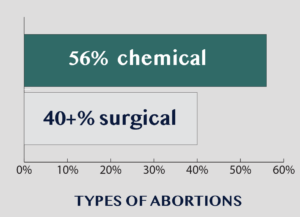
Today, abortion is divided between two types of procedures: chemical and surgical. More than half of abortions are now induced through taking two different prescription drugs over a period of several days. About 40% of abortions are done through a variety of surgical procedures.
What is the Cost for an Abortion?
Planned Parenthood is the biggest provider of abortion in America. The following is the information they provide the public online regarding abortion costs in their facilities.
“Abortion Pills (AKA medication abortion) can cost up to around $800, but it’s often less. The average cost at Planned Parenthood is around $580.
An in-clinic abortion can cost up to around $800 in the first trimester, but it’s often less. The average cost of a first trimester in-clinic abortion at Planned Parenthood is about $600. The cost of a second trimester abortion at Planned Parenthood varies depending on how many weeks pregnant you are. The average ranges from about $715 earlier in the second trimester to $1,500-2,000 later in the second trimester.”
The number of late term abortions, those occurring in the second and third trimesters of pregnancy (after 21 weeks), are rare and require different procedures and present substantive medical risks to the mother. There are only a handful of facilities in the United States willing to perform such procedures especially when the life or continuing health of the mother is not at risk if the pregnancy is carried to term. This is different from an emergency care situation where a pregnancy is lost by miscarriage or other fetal anomalies in the final trimester. No state in the Union prohibits abortion at any stage of the pregnancy if the life of the mother is at risk.
Furthermore, it is important to note that federal law requires any hospital that accepts federal Medicare funding to provide emergency medical treatment to any patient that enters that facility.
The law is called EMTALA, the Emergency Medical Treatment and Labor Act. This law applies to the mandatory provision of care regarding emergency abortions. The U.S. Supreme Court has upheld this law as recently as 2024.
How Many Abortions Do Women Have?